Adhesive capsulitis of shoulder
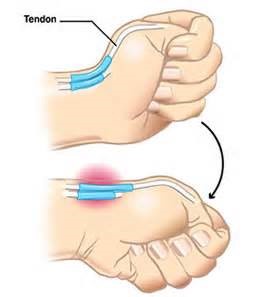
Frozen shoulder, medically referred to as adhesive capsulitis, is a disorder in which the shoulder capsule, the connective tissue surrounding the glenohumeral joint of the shoulder, becomes inflamed and stiff, and grows together with abnormal bands of tissue, called adhesions, greatly restricting motion and causing chronic pain.
Adhesive capsulitis is a painful and disabling condition that often causes great frustration for patients and caregivers due to slow recovery. Movement of the shoulder is severely restricted. Pain is usually constant, worse at night, and along with the restricted movement can make even small tasks impossible. Certain movements can cause sudden onset of tremendous pain and cramping that can last several minutes.
This condition, for which an exact cause is unknown, can last from 5 months to 3 years or more, and is thought in some cases to be caused by injury or trauma to the area. It may also appear for no apparent reason. It is also believed that it may have an autoimmune component, with the body attacking healthy tissue in the shoulder. The condition may also cause chronic inflammation. Adhesions grow between the joints and tissue, greatly restricting motion and causing a number of painful complications. There is also a lack of fluid in the joint, further restricting movement.
In addition to difficulty with everyday tasks, people who suffer from adhesive capsulitis usually experience problems sleeping for extended periods due to pain that is worse at night and restricted movement/positions, resulting in chronic fatigue and other complications. The condition also can lead to depression, pain and problems in the neck and back, as well as damage to the tissue surrounding the area.
There are a number of risk factors for frozen shoulder, including diabetes, stroke, accidents, lung disease, connective tissue disorders, and heart disease. The condition very rarely appears in people under 40.
Treatment is painful and taxing, and consists of physical therapy, various medications, massage therapy, and in severe cases, surgery. A doctor may also perform manipulation under anesthesia, which breaks up the adhesions and scar tissue in the joint to help restore some range of motion.
In approximately 15% of patients, adhesive capsulitis may appear in both shoulders, at different times or together.
Treatment is painful and taxing, and consists of physical therapy, various medications, massage therapy, and in severe cases, surgery. A doctor may also perform manipulation under anesthesia, which breaks up the adhesions and scar tissue in the joint to help restore some range of motion.
In approximately 15% of patients, adhesive capsulitis may appear in both shoulders, at different times or together.
Presentation:
Movement of the shoulder is severely restricted. The condition is sometimes caused by injury that leads to lack of use due to pain but also often arises spontaneously with no obvious preceding trigger factor. These seemingly spontaneous cases are usually referred to as Idiopathic frozen shoulder. Rheumatic disease progression and recent shoulder surgery can also cause a pattern of pain and limitation similar to frozen shoulder. Intermittent periods of use may cause inflammation.
Abnormal bands of tissue (adhesions) grow between the joint surfaces, restricting motion. There is also a lack of synovial fluid, which normally helps the shoulder joint move by lubricating the gap between the humerus (upper arm bone) and the socket in the scapula (shoulder blade). It is this restricted space between the capsule and ball of the humerus that distinguishes adhesive capsulitis from a less complicated, painful, stiff shoulder. People with diabetes, stroke, lung disease, rheumatoid arthritis, and heart disease, or who have been in an accident, are at a higher risk for frozen shoulder. Adhesive capsulitis has been indicated as a possible adverse effect of some forms of highly active antiretroviral therapy (HAART). The condition rarely appears in people under 40 years old and (at least in its idiopathic form) is much more common in women than in men (70% of patients are women aged 40-60). Frozen shoulder in diabetic patients is generally thought to be a more troublesome condition than in the non-diabetic population. If a diabetic patient develops frozen shoulder then the time to full recovery is often prolonged from the usual 12 month period. Cases have also been reported after breast or lung surgery.
Prevention:
To prevent the problem, a common recommendation is to keep the shoulder joint fully moving to prevent a frozen shoulder. Often a shoulder will hurt when it begins to freeze. Because pain discourages movement, further development of adhesions that restrict movement will occur unless the joint continues to move full range in all directions (adduction, abduction, flexion, rotation, and extension). Therapy will help one continue movement to discourage freezing and warm it. A medical doctor referral is needed before? physical therapy.
Signs and diagnosis:
With a frozen shoulder, one sign is that the joint becomes so tight and stiff that it is nearly impossible to carry out simple movements, such as raising the arm. People complain that the stiffness and pain worsen at night. Pain due to frozen shoulder is usually dull or aching. It can be worsened with attempted motion. A doctor, or therapist (occupational, massage or physical), may suspect the patient has a frozen shoulder if a physical examination reveals limited shoulder movement.
Frozen shoulder can also be diagnosed if limits to the active range of motion (range of motion from active use of muscles) are the same or almost the same as the limits to the passive range of motion (range of motion from a person manipulating the arm and shoulder). An arthrogram or an MRI scan may confirm the diagnosis – although in practice this is rarely required. Most orthopaedic specialists make the diagnosis of frozen shoulder by recognising the typical pattern of signs and symptoms.
Physicians have described the normal course of a frozen shoulder as having three stages:
- Stage one: The “freezing” or painful stage, which may last from six weeks to nine months, and in which the patient has a slow onset of pain. As the pain worsens, the shoulder loses motion.
- Stage two: The “frozen” or adhesive stage is marked by a slow improvement in pain, but the stiffness remains. This stage generally lasts four months to nine months.
- Stage three: The “thawing” or recovery, during which shoulder motion slowly returns toward normal. This generally lasts five months to 26 months.
Management:
Management of this disorder focuses on restoring joint movement and reducing shoulder pain. Usually, it begins with nonsteroidal anti-inflammatory drugs (NSAIDs).
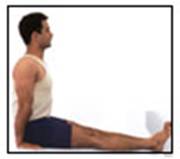
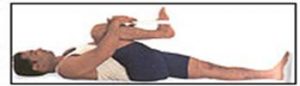
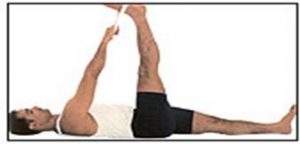
Physiotherapy treatments can help the situation. The treatment include interferential therapy, ultrasound, heat or cold therapy. Follow by gentle passive and active stretching exercises. These stretching exercises, which may be performed in the home with the help of a physiotherapist , are the treatment of choice. Treatment may be needed for several months.
If these measures are unsuccessful, the doctor may recommend manipulation of the shoulder under general anesthesia to break up the adhesions. Surgery to cut the adhesions is only necessary in some cases. Surgery to correct other problems with the shoulder may also be needed.